An in-depth exploration of the Endocannabinoid System — the biological network that was hiding in plain sight for most of human history, and why it may be one of the most important systems you've never heard of.
AB
Amrit Baral, PhD, MBBS, MPH
Physician-Scientist | Cannabis & Psychedelics Researcher
Postdoctoral Fellow · Johns Hopkins Bloomberg School of Public Health
Scroll
"After years of medical practice, public health research and studying cannabis and its effect on human health, the question I still get most often isn't about THC or CBD — it's simply: how does it all work? The answer begins inside every one of us."
— Amrit Baral · Introduction to ECS
Section 01 — The Basics
What Is the Endocannabinoid System?
Let me start with a confession: the endocannabinoid system (ECS) was only formally identified in the early 1990s. We had been studying cannabis for decades before we even knew this system existed inside us. It took the plant to help us find the biology.
The ECS is a complex cell-signaling system present in virtually all vertebrates. It is not a niche system tucked away in one organ — it is woven throughout your brain, organs, immune tissue, and connective tissue. It is one of the most widespread receptor systems in the entire human body, and its primary job is to maintain homeostasis — biological balance.
🌿 Plain Language — The Thermostat Analogy
Think of the ECS as your body's internal thermostat — but instead of regulating just temperature, it regulates dozens of biological "temperatures" simultaneously: your mood, your pain response, your appetite, your immune activity, your sleep cycles, and more. When something tips too far in one direction, the ECS kicks in to nudge it back toward center.
The Homeostasis Spectrum — ECS Works to Keep You Here
← TOO LITTLE (deficiency)(excess) TOO MUCH →
⚗️ Technical — Official Definition
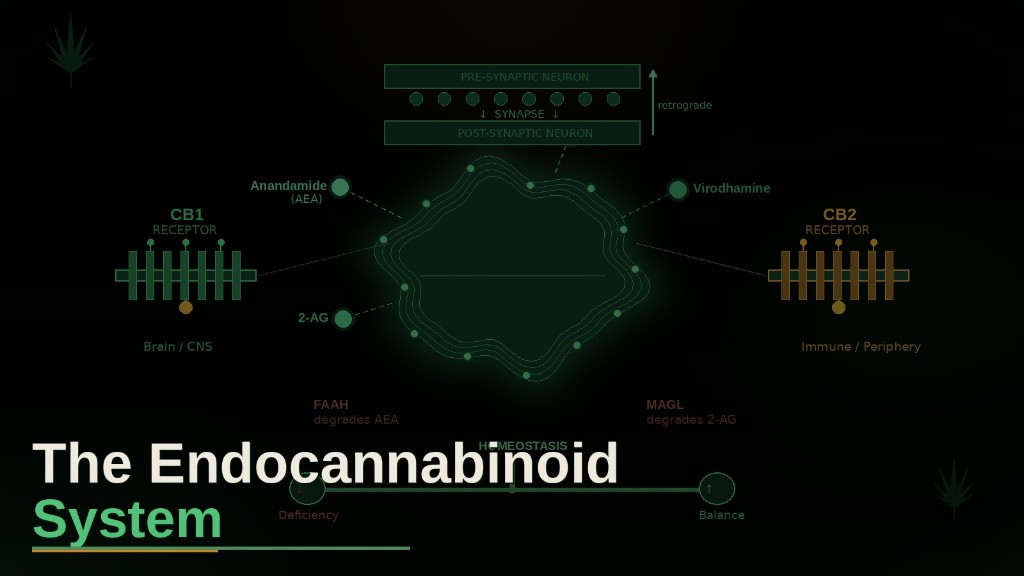
The ECS is defined as a lipid-based retrograde neurotransmitter system comprising endogenous cannabinoids (endocannabinoids), their metabolic enzymes, and their target receptors — primarily CB1R and CB2R. Unlike most neurotransmitters that travel forward across a synapse, endocannabinoids are synthesized on demand and travel backward (retrograde), providing inhibitory feedback to regulate synaptic transmission.
Section 02 — Discovery
A Brief History of a Late Discovery
Given how fundamental the ECS is, it is almost embarrassing that we only discovered it within my professional lifetime. Here is how the picture came together:
1964
THC Is Isolated
Dr. Raphael Mechoulam and his team in Israel isolate and synthesize delta-9-tetrahydrocannabinol (THC) — the primary psychoactive compound in cannabis. The question immediately becomes: how does it work in the body?
1988
First Cannabinoid Receptor Found
Allyn Howlett and William Devane discover the first cannabinoid receptor in rat brain tissue. The receptor's widespread presence in the brain immediately suggests something much bigger than just a drug target.
1990
CB1 Receptor Cloned
Lisa Matsuda's team at the National Institute of Mental Health successfully clones the CB1 receptor, allowing researchers to study it at the molecular level and confirming it as a distinct, purposeful receptor class.
1992
First Endocannabinoid Discovered — Anandamide
Mechoulam's team identifies the first endogenous cannabinoid: N-arachidonoylethanolamine, which they name anandamide from the Sanskrit word for bliss. The body makes its own cannabis-like compounds — the field is transformed forever.
1993
CB2 Receptor Identified
A second cannabinoid receptor, CB2, is discovered — primarily in immune tissue. This opens an entirely different dimension of the ECS, far beyond the brain.
1995
2-AG Identified
2-arachidonoylglycerol (2-AG), the second major endocannabinoid, is characterized. It is present in far higher concentrations than anandamide and binds fully to both CB1 and CB2 receptors.
2000s–Present
The Field Explodes
Thousands of studies across the globe reveal the ECS's role in pain, inflammation, neurogenesis, metabolism, fertility, cancer biology, and more. We are still, honestly, just scratching the surface.
Section 03 — The Three Pillars
The Three Core Components
The ECS is built on three pillars. Understanding each one is essential to understanding how the whole system works.
01
Endocannabinoids
The Messengers
Lipid-based molecules synthesized by your body on demand. They are the "keys" that activate the system's receptors. The two primary endocannabinoids are anandamide (AEA) and 2-arachidonoylglycerol (2-AG).
02
Receptors
The Locks
Protein structures embedded in cell membranes throughout the body. The two main types — CB1 and CB2 — receive endocannabinoid signals and translate them into cellular responses.
03
Metabolic Enzymes
The Cleanup Crew
Enzymes that synthesize endocannabinoids when needed and break them down once their job is done. Key enzymes include FAAH (breaks down anandamide) and MAGL (breaks down 2-AG).
🌿 Plain Language — The Lock & Key
Imagine your cells each have tiny locks on their surface. Your body produces keys (endocannabinoids) that fit those locks (receptors). When a key turns a lock, the cell receives a message: "slow down," "speed up," "stop firing," or "release this chemical." After the message is delivered, enzymes arrive like maintenance workers and remove the key so the lock is clear for the next signal.
Section 04 — The Receptors
CB1 & CB2: Two Receptors, Very Different Jobs
CB1
Cannabinoid Receptor Type 1
Predominantly found in the central nervous system (brain & spinal cord)
Highest concentration of any receptor in the brain
Mediates psychoactive effects of THC
Involved in pain modulation, memory, appetite, mood, and motor control
Also present in the liver, lungs, kidneys, and reproductive organs
Key target for understanding neurological conditions
CB2
Cannabinoid Receptor Type 2
Predominantly found in immune tissues and peripheral organs
High expression in spleen, tonsils, and immune cells
Does not produce psychoactive effects
Central role in inflammation and immune response regulation
Also found in the gut, bone marrow, and skin
Major focus of anti-inflammatory drug research
⚗️ Technical — G-Protein Coupled Receptors
Both CB1 and CB2 are G-protein coupled receptors (GPCRs). When activated, they primarily couple to Gi/o proteins, leading to inhibition of adenylyl cyclase, reduction of intracellular cAMP, and modulation of ion channel activity. CB1 activation typically reduces neuronal excitability by inhibiting voltage-gated calcium channels and activating inwardly rectifying potassium channels — explaining its broad inhibitory and modulatory effects on neurotransmission. Researchers have also identified additional endocannabinoid targets beyond CB1/CB2, including GPR55, GPR18, TRPV1, and certain PPAR nuclear receptors.
Section 05 — The Molecules
Your Body's Own Cannabinoids
One of the most remarkable facts about the ECS is that your body makes its own versions of the active compounds found in cannabis. These molecules — endocannabinoids — are not stored and released like most neurotransmitters. They are synthesized on demand, do their work, and are then immediately broken down.
You've heard of the "runner's high" — that feeling of euphoria and reduced pain during intense exercise. For years, we assumed it was entirely caused by endorphins. Recent research strongly suggests that anandamide — your body's own cannabis-like molecule — plays an equal or even greater role in producing this state. Your body has been making its own natural bliss compound all along.
Section 06 — Clinical Significance
Where the ECS May Matter Most
Because the ECS is involved in so many fundamental physiological processes, disruption or deficiency of ECS function has been proposed as a contributing factor in a wide range of conditions. The field of "Clinical Endocannabinoid Deficiency" (CECD), first proposed by Dr. Ethan Russo in 2001, suggests that low endocannabinoid tone may underlie conditions such as:
A note on where the science stands — and where it still needs to go: The associations listed above range from well-supported to preliminary, and it is important to hold them honestly. Some, like the ECS's role in pain modulation and epilepsy, are backed by robust clinical trial data and have already translated into approved therapeutics. Others — particularly in neurodegenerative disease, autism spectrum disorders, and metabolic conditions — remain largely at the preclinical or early-phase human trial stage. Animal models are promising, but they are not people. Correlation in observational data is not causation. And anecdote, however compelling, is not evidence.
As a researcher, I find the ECS one of the most exciting therapeutic frontiers in modern medicine. As a physician, I am equally obligated to say: we need more. More large-scale, placebo-controlled human trials. More longitudinal data on long-term ECS modulation. More research into dosing, receptor selectivity, and population-specific responses — particularly in women, older adults, and people with complex comorbidities who are chronically underrepresented in cannabinoid research. The science is real and growing, but it is not yet complete. Anyone who tells you otherwise — whether they are dismissing the ECS entirely or promising it as a cure-all — is not giving you the full picture. The honest position is one of rigorous optimism: the evidence is strong enough to take seriously, and incomplete enough to keep working.
Section 07 — Plant Compounds
How Cannabis Interacts with Your ECS
Cannabis contains over 100 identified phytocannabinoids — plant-derived compounds that interact with the ECS. They work because our receptors are structurally receptive to them, not because the plant evolved to "hack" our biology, but because our biology and the plant's chemistry arrived at a remarkable molecular coincidence over millions of years of evolution.
THC
Delta-9-Tetrahydrocannabinol
Partial agonist at CB1 and CB2. Produces psychoactive effects via CB1. Also has analgesic, anti-nausea, and appetite-stimulating properties.
CBD
Cannabidiol
Non-intoxicating. Acts as a negative allosteric modulator at CB1. Also interacts with TRPV1, serotonin receptors, and inhibits FAAH — raising anandamide levels.
CBG
Cannabigerol
The "mother cannabinoid" — precursor to THC and CBD. Partial agonist at CB1/CB2. Studied for antibacterial, anti-inflammatory, and neuroprotective effects.
CBN
Cannabinol
Weakly psychoactive degradation product of THC. Moderate CB2 affinity. Studied for sedative properties and possible bone-stimulating effects.
THCV
Tetrahydrocannabivarin
At low doses, acts as a CB1 antagonist (opposite of THC). At higher doses, may activate CB1. Studied for appetite suppression and potential in diabetes management.
⚗️ Technical — The Entourage Effect
A concept formalized by Dr. Raphael Mechoulam and expanded by Dr. Ethan Russo, the entourage effect proposes that phytocannabinoids, terpenes, and flavonoids work synergistically — producing effects greater than any single compound in isolation. For example, the terpene β-caryophyllene is a selective CB2 agonist, meaning it directly activates the ECS. This suggests that whole-plant preparations may have therapeutic advantages over isolated compounds — a hypothesis that continues to be rigorously tested in clinical settings.
Section 08 — Practical Application
Supporting Your ECS Without Cannabis
One of the most empowering insights from ECS research is that you do not need cannabis to support this system. Lifestyle factors profoundly influence your endocannabinoid tone — something I always emphasize to my students and patients.
Exercise
Aerobic exercise elevates circulating anandamide levels. The runner's high is real and endocannabinoid-mediated. Even a moderate walk has been shown to positively shift endocannabinoid tone.
Omega-3 Fatty Acids
Endocannabinoids are synthesized from arachidonic acid, an omega-6 fatty acid. Omega-3 fatty acids (found in fish, flaxseed, and walnuts) help maintain the right omega-6 to omega-3 ratio, supporting healthy endocannabinoid signaling. Chronic omega-3 deficiency has been linked to impaired ECS function.
Stress Reduction
Chronic stress depletes anandamide and disrupts ECS homeostasis. Mindfulness practices, yoga, breathwork, and adequate sleep all support ECS recovery. The ECS and the HPA (stress) axis are in constant dialogue.
Social Connection & Osteopathic Manipulation
Social bonding elevates anandamide. Massage, acupuncture, and certain osteopathic techniques have been shown to modulate endocannabinoid signaling — which may partly explain why physical touch is so therapeutic.
Intermittent Fasting
Caloric restriction and fasting appear to upregulate CB1 receptor density and modulate endocannabinoid levels — a fascinating crossroads between metabolic research and cannabinoid science.
🌿 Plain Language — A System You Already Tend To
Every time you take a morning run, eat a handful of walnuts, hug someone you love, or get a full night of sleep — you are already supporting your endocannabinoid system. Cannabis is one way to interact with this system, but it is far from the only way. The ECS responds to how you live your life, every single day.
Section 09 — Final Thoughts
The Most Important System You Were Never Taught About
I have spent 19 years in medicine, public health, and research — and the endocannabinoid system still astonishes me. My entire doctoral work was devoted to understanding the effects of cannabis and psychedelics in cancer: how these compounds interact with the body at the cellular level, how they modulate pain and inflammation, and why patients who had been dismissed by conventional medicine were finding relief through pathways that mainstream science had barely begun to map. At the center of nearly every finding was the ECS.
We are still uncovering new receptor subtypes, new endocannabinoids, new mechanisms, and new therapeutic possibilities with every passing year. The tragedy is not the complexity — science thrives on complexity. The tragedy is how little this system is taught in standard medical and biology education.
I know this firsthand. I was never introduced to the endocannabinoid system in medical school. I learned every other major biological system — the cardiovascular, the endocrine, the immune, the autonomic nervous system — in painstaking detail. But the ECS? Not a single lecture. Not a single slide. A system that governs pain, mood, memory, appetite, inflammation, and neuroplasticity, and it was entirely absent from my medical training. I only encountered it through my own research, years later, when I began asking questions that clinical medicine had no satisfying answers to.
Ask most physicians about the endocannabinoid system today and you will often still be met with a blank stare — or worse, a dismissive response rooted in the politics of cannabis prohibition rather than the weight of scientific evidence. That is beginning to change, but far too slowly. The stigma surrounding cannabis has cast a long shadow over one of the most important discoveries in modern biology, and patients have paid the price in unaddressed pain, undertreated conditions, and missed therapeutic windows.
My hope is that every person who reads this walks away with one core understanding: you were born with a cannabis-like system inside you. It is not a foreign imposition from a plant — it is a fundamental, ancient part of what makes you, biologically, human. Understanding the ECS is not just about understanding cannabis or psychedelics. It is about understanding one of the central regulatory architectures of life itself — and reclaiming the science that should have been taught to every physician, every nurse, and every patient from the very beginning.
"The endocannabinoid system did not evolve to process a plant. It evolved to process life — and that is exactly why it matters so much."
— Amrit Baral, PhD, MBBS, MPH
Medical Disclaimer: This article is written for educational purposes only and reflects current scientific research and the author's expert interpretation thereof. Nothing in this article constitutes medical advice. Cannabis and cannabinoid-based therapies are subject to varying legal statuses by jurisdiction. Always consult a qualified healthcare provider before making any medical decisions. Research in this field is ongoing, and this article reflects the state of knowledge as of its publication date.